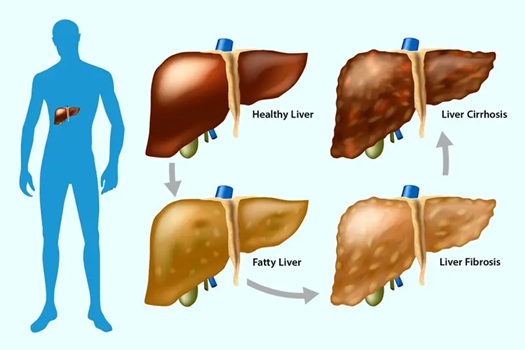
Your liver is one of the most resilient organs in your body, capable of regenerating even after significant damage. Yet, when fat accumulates in liver cells, it can trigger a cascade of events that leads to scarring—medically known as fibrosis. In severe cases, this scarring progresses to cirrhosis, where the liver becomes so damaged it can no longer function properly.
But why does fat, a substance your body uses for energy, cause such harm to the liver?
Dealing with this process is crucial, as fatty liver disease affects approximately one in four adults globally and is rapidly becoming one of the leading causes of liver failure. Let’s explore the complex biological mechanisms that transform a healthy liver into a scarred, dysfunctional organ.
The Liver’s Normal Role in Fat Metabolism
To understand what goes wrong, we first need to appreciate what the liver does normally. Your liver is the body’s primary metabolic command centre, processing nutrients from everything you eat and drink. Among its many functions, the liver:
- Breaks down fats from your diet
- Packages fats for transport throughout the body
- Converts excess carbohydrates and protein into fat for storage
- Produces bile to help digest dietary fats
- Regulates blood sugar by storing and releasing glucose
In a healthy person, the liver contains minimal fat—typically less than 5% of its weight. When fat accumulation exceeds this threshold, the stage is set for potential damage.
Stage One: Fat Accumulation (Steatosis)
The journey toward liver scarring begins innocuously with simple fat accumulation, or steatosis. This occurs when the liver takes in more fat than it can process and export, leading to fat droplets accumulating inside liver cells (hepatocytes).
Several factors drive this accumulation:
- Excess Caloric Intake: Consuming more calories than you burn—particularly from refined carbohydrates, sugars, and alcohol—leads to increased fat production in the liver.
- Insulin Resistance: When cells become resistant to insulin (common in obesity and metabolic syndrome), the liver responds by producing more fat while simultaneously becoming less efficient at exporting it.
- Dietary Fructose: High fructose consumption, particularly from added sugars and high-fructose corn syrup, is uniquely problematic. Unlike glucose, fructose is metabolized almost exclusively in the liver, where it’s readily converted to fat.
- Alcohol Metabolism: The liver processes alcohol into toxic byproducts that directly promote fat accumulation while impairing the liver’s ability to export fats.
At this stage, the liver may be enlarged and fatty, but there’s typically no inflammation or damage. Many people with simple steatosis have no symptoms and may not even know they have the condition. For some individuals, fatty liver remains at this stage indefinitely without progressing further.
However, for others—and scientists don’t fully understand why some people progress while others don’t—the accumulation of fat triggers a more dangerous cascade.
Stage Two: Inflammation and Oxidative Stress
The critical transition from benign fat accumulation to liver damage involves inflammation. When liver cells become overloaded with fat, several harmful processes begin:
Lipotoxicity
Fat itself, particularly certain types of fatty acids, becomes toxic to liver cells when present in excessive amounts. This “lipotoxicity” occurs through multiple mechanisms:
- Mitochondrial Dysfunction: Fat-laden liver cells struggle to process all the fatty acids flooding into their mitochondria (the cellular energy factories). This overwhelms the mitochondria, causing them to produce excessive amounts of reactive oxygen species (ROS)—highly reactive molecules that damage cellular structures.
- Endoplasmic Reticulum Stress: The endoplasmic reticulum, responsible for protein and fat processing, becomes overwhelmed by the excess fat. This triggers a stress response that, when chronic, leads to cell damage and death.
- Cellular Membrane Damage: Certain fatty acids can directly damage cell membranes, particularly when oxidised. This compromises the integrity of liver cells, making them more vulnerable to injury.
Inflammatory Response
As liver cells become damaged and die, they release signals that activate the immune system. Immune cells flood into the liver, releasing inflammatory molecules called cytokines. This inflammation is the body’s attempt to clear away damaged cells and initiate repair—but when it becomes chronic, inflammation itself becomes part of the problem.
Key inflammatory mediators include:
- Tumour necrosis factor-alpha (TNF-α)
- Interleukins (IL-6, IL-1β)
- Transforming growth factor-beta (TGF-β)
These inflammatory signals not only damage liver cells directly but also activate the cells responsible for creating scar tissue.
Oxidative Stress
The combination of mitochondrial dysfunction and inflammation creates a state of oxidative stress, where harmful ROS overwhelm the liver’s antioxidant defences. These reactive molecules damage DNA, proteins, and fats throughout liver cells, accelerating cell death and inflammation in a vicious cycle.
Stage Three: Fibrosis (Scarring)
Here’s where permanent damage begins. As inflammation persists, specialised cells called hepatic stellate cells become activated. In a healthy liver, these cells remain dormant, but inflammation and liver cell death wake them up, transforming them into scar-producing factories.
The Stellate Cell Transformation
Activated stellate cells undergo a dramatic transformation:
- They multiply rapidly
- They begin producing large amounts of collagen and other extracellular matrix proteins
- They contract, making the liver stiffer
- They produce more inflammatory signals, perpetuating the damage
The collagen they produce is meant to be temporary scaffolding while the liver repairs itself. However, in chronic fatty liver disease, the repair signal never turns off. The stellate cells keep producing collagen, and scar tissue gradually replaces normal liver tissue.
The Scar Tissue Cascade
Several factors drive this scarring process:
- Persistent Inflammation: As long as fat accumulation continues and liver cells keep dying, inflammation persists, keeping stellate cells activated and producing collagen.
- TGF-β Signaling: This powerful pro-fibrotic cytokine is released by damaged liver cells and immune cells. It’s the master regulator of fibrosis, directly stimulating stellate cells to produce more scar tissue.
- Impaired Matrix Breakdown: Normally, the body can break down and remove excess collagen through enzymes called matrix metalloproteinases (MMPs). However, in chronic liver disease, inhibitors of these enzymes (TIMPs) increase, preventing normal scar tissue removal.
- Microcirculation Damage: As scar tissue accumulates, it disrupts the liver’s blood supply. This creates areas of low oxygen (hypoxia), which further activate stellate cells and promote scarring.
Why Scarring Is Problematic
Unlike normal liver tissue, scar tissue doesn’t perform any liver functions. As scarring progresses:
- Blood flow through the liver becomes restricted, increasing pressure in the portal vein (portal hypertension)
- Remaining healthy liver cells must work harder to compensate
- The liver’s ability to perform its vital functions—detoxification, protein synthesis, bile production—gradually declines
- The scarred, stiff liver can’t regenerate normally when additional damage occurs
Stage Four: Advanced Fibrosis and Cirrhosis
If fat accumulation and inflammation continue unchecked, fibrosis progresses through stages:
- Stage 1-2 (Mild to Moderate Fibrosis): Scar tissue forms around blood vessels and in specific zones of the liver. At this stage, the scarring is potentially reversible with aggressive intervention.
- Stage 3 (Advanced Fibrosis): Scar tissue forms bridges between different areas of the liver, significantly disrupting architecture. Reversal becomes more difficult but may still be possible.
- Stage 4 (Cirrhosis): Extensive scarring completely distorts liver structure. The organ becomes nodular, stiff, and largely dysfunctional. At this stage, scarring is generally considered irreversible.
Cirrhosis creates a dangerous situation where the liver can no longer adequately perform its vital functions, leading to complications like:
- Fluid accumulation (ascites)
- Brain dysfunction from toxin buildup (hepatic encephalopathy)
- Bleeding disorders
- Increased risk of liver cancer
- Eventually, liver failure requiring transplantation
Why Some People Progress While Others Don’t
Not everyone with fatty liver develops inflammation and fibrosis. Several factors influence progression:
- Genetic Factors: Certain genetic variants (like PNPLA3 and TM6SF2) increase susceptibility to progression from simple steatosis to fibrosis.
- Metabolic Health: The presence of diabetes, obesity, and metabolic syndrome dramatically increases risk of progression.
- Additional Hits: Concurrent factors like alcohol use, viral hepatitis, certain medications, or environmental toxins accelerate damage.
- Duration: The longer fat remains in the liver, the higher the risk of progression. This is why early intervention is crucial.
- Gut Health: Emerging research suggests the gut microbiome plays a role, with certain bacterial populations potentially promoting or protecting against liver inflammation.
Breaking the Cycle: Prevention and Reversal
The good news is that liver fibrosis—even at moderate stages—can potentially be reversed if the underlying cause is addressed:
Primary Interventions
- Weight Loss: Even modest weight reduction (7-10% of body weight) can significantly reduce liver fat and inflammation, potentially reversing early fibrosis.
- Dietary Changes: Reducing refined carbohydrates, added sugars, and saturated fats while increasing fiber, healthy fats, and plant-based foods supports liver health.
- Exercise: Regular physical activity improves insulin sensitivity and reduces liver fat independent of weight loss.
- Alcohol Abstinence: For alcoholic fatty liver disease, complete abstinence is essential.
- Managing Metabolic Conditions: Controlling diabetes, high cholesterol, and high blood pressure reduces the “additional hits” that accelerate liver damage.
Emerging Supportive Therapies
While lifestyle modification remains the cornerstone of treatment, several interventions show promise in supporting liver health:
- Peptide Therapy: Certain peptides may support liver health through various mechanisms. Growth hormone-secreting peptides like Ipamorelin can improve metabolic health and insulin sensitivity, addressing root causes of fat accumulation. BPC-157 has demonstrated anti-inflammatory and healing properties that may support liver tissue repair, though specific liver research is limited.
- Antioxidant Support: Compounds that reduce oxidative stress—like vitamin E, milk thistle, and N-acetylcysteine—may help protect liver cells from damage, though results are mixed.
- GLP-1 Agonists: These medications, which reduce appetite and improve metabolic health, have shown promise in reducing liver fat and inflammation in clinical trials.
- Anti-inflammatory Approaches: Addressing systemic inflammation through diet, stress management, sleep optimisation, and potentially targeted supplements may help reduce the inflammatory drive behind fibrosis.
The Importance of Early Detection
Because fatty liver disease is often silent until advanced stages, screening is crucial for those at risk:
- People with obesity or overweight
- Those with type 2 diabetes or prediabetes
- Anyone with metabolic syndrome
- People who consume excessive alcohol
- Individuals with elevated liver enzymes on routine bloodwork
Early detection allows intervention before irreversible scarring develops. Regular monitoring through blood tests, imaging studies, and in some cases, specialized scans that measure liver stiffness can track disease progression or improvement.
Avoid Scar Tissue
Fat causes liver scar tissue through a complex cascade: excess fat accumulation leads to cellular stress and toxicity, triggering inflammation and oxidative damage. This chronic inflammation activates stellate cells that produce collagen, gradually replacing functional liver tissue with non-functional scar tissue. Left unchecked, this process progresses to cirrhosis and liver failure.
However, understanding this pathway also reveals opportunities for intervention. By addressing the root causes—excess fat accumulation, insulin resistance, inflammation—through lifestyle modification and potentially supportive therapies like metabolic peptides, many people can halt or even reverse this progression.
Your liver is remarkably resilient, but it needs your help. The choices you make today—what you eat, how you move, whether you address metabolic dysfunction—determine whether your liver remains healthy or progresses down the path toward scarring and failure.